






















The Moose River home that Skyler Carpenter pulls up to in his Ford F-150 paramedic truck is familiar to him.
He’s been there on several occasions to draw blood from the owner of the home, 91-year-old Marcelle Lumbert, to check her medications or to offer other medical aid.
But he was back on a frigid winter night because Lumbert had become light-headed and fell in her bathroom. Her two sons live nearby and found her on the floor when they stopped by to check on her.
Carpenter sat across from Lumbert on the edge of her bathtub as he assessed her. She rested her hands on her knees with black tape covering the left lens of her glasses because of a persistent eye problem.
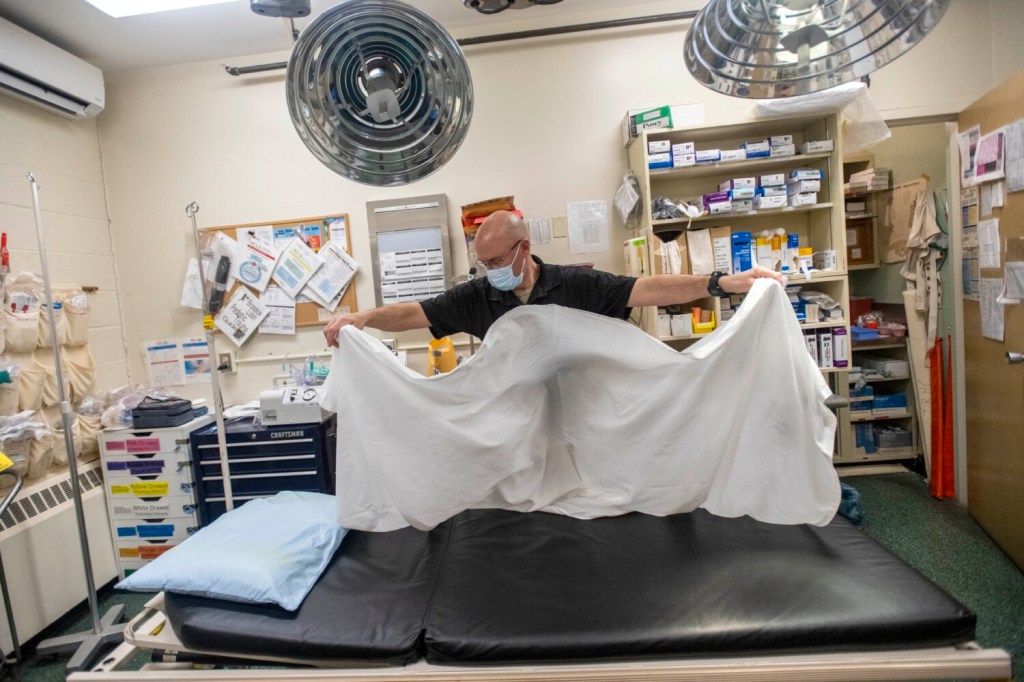
Marcelle Lumbert is helped to her feet by paramedic and community health practitioner Skyler Carpenter in her bathroom after she fainted in the late evening hours Dec. 12, 2021, in Moose River. Michael G. Seamans/Morning Sentinel
Lumbert, who’s lived all her life in either Moose River or next door in Jackman, is lucky to have Carpenter looking after her. Up until recently, such a fall would have likely sent her to the closest hospital — an hour-and-a-half away at Redington-Fairview General Hospital in Skowhegan.
Carpenter was an EMT for Scarborough-based North East Mobile Health Services with more than 20 years of experience in the back of an ambulance. But he recently completed a broader level of training that gives him the title of physician extender.
He’s now able to use cardiac machines, is well-versed in serious cardiac events and can make a variety of medical determinations either on his own or in consultation with an on-duty physician at a partnering hospital. All of this is the result of a program being rolled out called the Critical Access Physician Extender Program, which gives paramedics the hospital training needed to provide emergency care procedures.
The program is a response to the decision in 2017 to end 24/7 on-call emergency care at Jackman Community Health Center. It’s also a reflection of how rural health care is transforming as critical care centers close and are now commonly found in more populated areas.
The venture, funded in part by an early $1.2 million federal grant, is a partnership involving North East Mobile Health, Penobscot Community Health Care, the town of Jackman and Bangor-based St. Joseph Healthcare. It seeks to provide a new model for health care delivery in rural areas for less money and better patient care.
Damian Brockway, a paramedic with North East Mobile Health, draws blood from Mary Rita Griffin, 97, on July 26, 2021, at her Jackman home. The biggest change in duties from an advanced EMS provider to the new community care practitioner is the extended care of regular patients versus the several emergency calls per shift in a normal paramedic environment. Michael G. Seamans/Morning Sentinel
Rick Bridges is a builder who has lived in Jackman about 20 years, having moved there from southern Maine for its remote lifestyle and “slower pace.” He was taken to the Jackman Community Health Center last year after suffering a deep cut to a finger. He said the nascent program helps provide some stability, and sense of relief, for the fewer than a thousand people who live in Jackman and a few hundred more in the broader region.
“I think for us and other people it’s definitely a little bit of security knowing there’s someone who can at least triage you and help you and possibly save your life, possibly save a limb,” Bridges said. “Without it I think there’d be a lot less people in town … So having something, as far as medical care, will keep people safer, securer and possibly alive longer depending on the situation.”
MEDICAL RESOURCES IN DECLINE
The need for the program, and its benefits, can be explained through the perspective of three people: Jackman-based Dr. Patricia Doyle; Dr. Jonnathan Busko, the medical director for service and consulting at the Jackman Community Health Center and an emergency physician for St. Joseph Hospital in Bangor; and Rick Petrie, chief operations officer for North East Mobile Health.
Doyle said a solution was needed to address declining medical resources in rural Somerset County.
Dr. Patricia Doyle examines Dennis Palmer during an acute care visit July 26, 2001, at the Penobscot Community Health Care clinic in Jackman. Michael G. Seamans/Morning Sentinel
“When I was hired on, the model was there are two providers and we would share the office hours and the call. And the reason that you needed the two providers was because when you have got 24/7 on-call, you can’t have one person doing that. It’s just not sustainable.”
— Dr. Patricia Doyle
After medical school at Tufts University and a residency at the former Maine Dartmouth Family Medicine in Waterville, Doyle found her way north to Jackman in the mid-1970s on a National Health Service Scholarship to pay for her medical school expenses by working as a physician in underserved areas. She and her husband liked the way of life, started a family and decided to stay.
The hospital in Jackman delivered its last baby decades ago and then became a nursing home, ultimately closing in 2017 because of deep financial losses. As services diminish and costs continue to grow, the town could ultimately have no clinic at all.
“When I was hired on, the model was there are two providers and we would share the office hours and the call,” Doyle said. “And the reason that you needed the two providers was because when you have got 24/7 on-call, you can’t have one person doing that. It’s just not sustainable.”
Enter Dr. Busko.
The CAPER program, which has been in the works for nearly four years, was derived from Busko’s experience working in Alaska.
He spent time in that state in the early 2000s and began developing the outline of a program to address staffing demands in delivering health care to a rural population. One answer was to expand the training of paramedics to provide a broader range of care, while giving the paramedics access to telemedicine so that doctors can be consulted about patient treatment.
“I knew what the community health practitioners were capable of, I knew where the holes in their training were,” Busko said. “By giving a paramedic that additional training, you would have a very high-functioning independent practitioner supported by telemedicine.”
Damian Brockway, a paramedic with Northeast Ambulance, practices placing a breathing tube at the Penobscot County Health Center in Jackman on May 8, 2021. Michael G. Seamans/Morning Sentinel
He said the model makes financial sense: It’s difficult to find doctors and physician assistants to work in rural settings, and paying them can be expensive, so giving paramedics greater training and access to doctors for long-distance consultations can be a sound solution.
Petrie, the program director for North East Mobile Health, said the Jackman program is driven by Busko’s ideas and experience.
“He has a really strong need to develop programs in rural areas like this to serve the underserved,” Petrie said. “He’s been the driving force here behind this. And he recognizes that in rural Maine … the health care system doesn’t reach a fair amount of people.”
Petrie said the program is designed for places that “are a long way away from a primary care hospital with an emergency room.”
“This paramedic would have little or no role as it’s structured right now in Portland, for instance, because they are close to a hospital with rapid transport time,” Petrie said. “Now there are other things Portland may be able to do along the lines of a community paramedicine kind of thing. But this model wouldn’t fit there.”
‘THERE’S ANOTHER PATHWAY’
Paramedicine, which integrates paramedics into the delivery of emergency medical services, got a boost in Maine in 2012 with legislation that allowed for paramedicine programs in places where health care services were lagging.
But Petrie said paramedicine hasn’t taken off in Maine because there isn’t a stable funding mechanism for it. So ambulance services that were doing it, “were doing it out of the kindness of their hearts,” Petrie said. “And they were eating the cost on it. And the thing is, eventually the people that pay the bills will realize that a strong paramedicine program can save them a bunch of money as well as provide better service to the patients.”
Damian Brockway, a paramedic and community health practitioner with Northeast Ambulance, sutures the finger of Rick Bridges as Andrea Groft, left, the per diem physician assistant, watches July 3, 2021, at the Penobscot County Health Clinic in Jackman. In the current model, the clinic is staffed with per diem physician assistants to expand the scope of practice available at the clinic. That care can be extended via a telemedicine visit with a doctor and the paramedic will perform whatever medical procedure is required. Michael G. Seamans/Morning Sentinel
He explained that the traditional reimbursement model for emergency medical services is based on transporting patients by ambulance to a hospital.
“Medicare and Medicaid are the primary payers in the state of Maine and nationally, and their reimbursement probably falls in the 85% range of what it costs to actually do a call,” Petrie said. “So it makes it really hard to pay EMS providers what they’re worth and that also makes it hard to retain them.”
And that’s particularly problematic in rural regions that are generally seeing a declining number of EMS workers and aging all-volunteer EMS stations.
“A model like this, we can say to a community, we can provide this for you, but we bill the increased pay rates into those costs so that paramedics and EMTs who are working those projects can get paid more money,” Petrie said.
“And I think those kind of opportunities really all of a sudden open the door to people saying, ‘Oh wow, there’s another pathway. I can go in when I’m young and energetic and work on an ambulance and bang these calls out and do these trips. But then once I get some experience under my belt, here are some alternative pathways,’” he said.
Send questions/comments to the editors.

Comments are no longer available on this story